Firefighter Cruz and Driver/Operator/Engineer Smith were sitting around the kitchen table drinking their coffee waiting on the morning briefing. They knew something was wrong. Captain Jones had been on the phone in his office most of the morning. He was hardly ever late to the morning briefing. When the captain finally emerged from his office, it was clear it had been an unpleasant conversation. Smith eventually mustered up enough courage to ask,
“Captain, do you want to tell us what is going on?”
Captain: I just got off the phone with the EMS chief, and it seems that Firefighter Thomas did a very poor job of documenting the patient care report for the heart attack patient we had last shift. I did not catch it.
Smith: Oh, how bad is it?
Captain (taking a deep sigh): He did not document that we did a 12-lead ECG.
Cruz (interrupting): Wait a minute; I did the 12-lead. It was a massive anterior infarct.
Captain: I know you did; but, unfortunately, it is not documented, so it might as well not have happened. It gets worse. Sullivan did not document any of the medications we administered.
Smith: Oh boy! I know we gave at least one round of nitroglycerin and some aspirin, but I can’t remember how many rounds we gave.
Everybody in the room had that sinking feeling in their gut.
Smith: Well, Captain, I am upset with Thomas for writing such a bad report; but, honestly, how did you miss all this when you reviewed the report?
Captain (looking down and then at his crew): I gave the report a quick glance over and told him to submit it. Truth be told, I have always trusted my folks to write a good patient care report. I have never really paid that much attention to the quality and accuracy of the report, but I guess that is going to have to change.
This scenario could happen in nearly any fire-based emergency medical services (EMS) organization. The importance of quality assurance (QA) at the officer level is often overlooked. QA should start at the company officer level. The station officer needs to evaluate and approve all patient care reports (PCRs) before they are submitted. QA should not be left completely up to an EMS chief or an outsourced third party. Company officers are responsible for ensuring that all PCRs written by their personnel are accurate and professionally written and meet the expectations of the department and medical control.
The Problem
The problem here is that few departments provide QA training to their officers. This lack of training creates ambiguity and a lack of consistency in how PCRs are reviewed. Officers can either pick apart the PCR for every small error or give the report a quick glance over. If Jones had an established plan and the necessary tools needed to review the PCR, he would not have missed such important information. He would have caught the errors, and the report would have been corrected before it was submitted.
PCRs can be divided into two general categories: handwritten reports and electronic patient care reports (ePCRs). The trend is moving away from handwritten reports, but some departments still use them. The QA process at the officer level for handwritten reports is very challenging. No automated programs flag potential issues as they do for ePCRs. The station officers must rely on their medical understanding and training for QA. This leads to ambiguity and inconsistencies in how reports are reviewed.
A Solution: QA Check Sheet
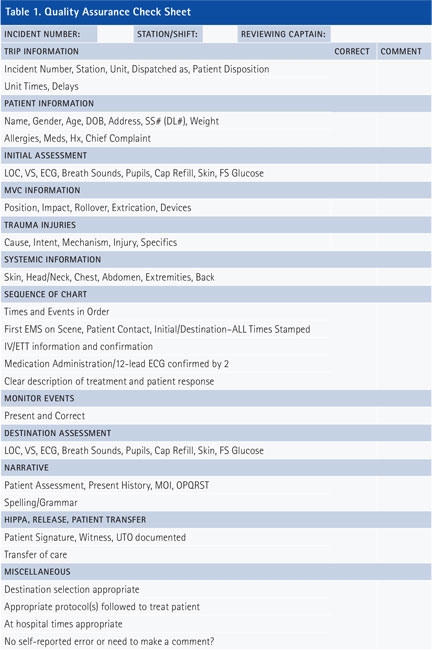
To ensure consistency, departments need to establish a standard QA procedure for company officers to follow. This will remove any inconsistencies and inform all personnel of what is expected through the QA process and what criteria should be included in the PCR. Table 1 shows a generic check sheet a company officer could use to assess the QA of a handwritten PCR. By following this check sheet, the company officer makes sure that the PCR meets the standards of the department and medical control.
Handwritten PCRs
When the PCR is ready for review, the officer can compare the report with the check sheet. If the information is present and correct, the officer marks “Correct” on the check sheet. If any information is incorrect or not included, the officer marks “Incorrect.” Once the officer is finished with the QA check sheet, it is handed back to the individual responsible for the PCR to make any corrections. If no corrections are needed or after the necessary corrections have been made, the PCR is ready for submission. The check sheet should be submitted with the PCR to the responsible party.
Electronic PCRs
The dynamics of the QA process at the company officer level are modified for ePCRs. Electronic reports are slightly easier to check for QA because automated programs flag potential issues. These automated features used in conjunction with a QA check sheet provide company officers with a consistent, systematic QA process. Although a variety of ePCRs exist and each has its own QA features, nearly all follow the same QA process.
The main QA features for ePCRs are some components of report validation. Report validation requires certain information to be input in the PCR before it can be submitted. These lockout fields or closed-call rules keep reports that do not contain the required information from being submitted-for example, if a medication is listed as being administered, a closed-call rule can be created to require that the dose and administration route be included before the report can be submitted. These types of closed-call rules keep paramedics from making basic oversights and assist the officer with QA. Report validation can be customized to some degree to fit each department’s needs.
Officers need to use report validation in conjunction with the QA check sheet. Closed-call rules require information to be input but are not able to verify the accuracy of the information. Inaccurate information will satisfy closed-call rules. For example, if the wrong medication, dose, or route is listed in the PCR, the rules cannot recognize or flag the inaccuracy. In addition, if information is omitted from the report, certain closed-call rules will not be triggered.
The company officer must have a systematic approach to identifying inaccurate information or omissions. He can use the QA check sheet with ePCRs, just as he does for handwritten reports. When the report is ready for review, the company officer can compare the report with the check sheet. Once the PCR meets the check sheet criteria and the report validation rules, the company officer can feel confident that the PCR meets the standards of the department and medical control.
Check Sheet Unique to Department
Regardless of whether the PCR is handwritten or an ePCR, a check sheet must be modified to fit the department’s process. For example, it should be adjusted to follow the PCR template order; the items on the check sheet should match the information in the PCR in a sequential order. This allows the officer to follow the information in the PCR and systematically match the correct fields on the check sheet.
One of the most important fields on the check sheet is the one for self-reporting errors. Mistakes happen. Fire-based EMS organizations must create an environment where mistakes are acknowledged and addressed in a productive manner. When mistakes are self-reported, discipline should be removed from the process. This does not mean that additional training or education is not warranted to ensure the mistake does not happen again. The objective is to create an environment where personnel will voluntarily admit their mistakes. This is a much more productive environment than one in which personnel hide their errors and hope that they will not be discovered.
Company officers are the first step in the QA process. They are responsible for all PCRs submitted by their personnel. Instead of having a documentation error that omits information from the PCR, as in the case with Jones at the beginning of this article, the omission would be caught before the report is submitted. If poor care was provided, the company officer is responsible for addressing the issue before submitting the report. If Jones had followed the check sheet, he would have caught the documentation mistakes before the report was submitted. Having a standardized QA process at the company officer level addresses issues in a proactive manner rather than handling them retroactively after the PCR has been submitted.
CASEY McCASLIN, a 14-year veteran of the fire service, is a battalion chief with the Allen (TX) Fire Department. He has a master of public affairs degree and a B.S. degree in biology and is an Executive Fire Officer alumnus. He is a licensed paramedic and certified to the technician level in rope rescue, confined space, and trench. He formerly taught EMS at Collin College.
Fire Engineering Archives

