FORGOTTEN FRACTURE
VEHICLE EXTRICATION
This extrication method will help reduce your rescue time, increase safety, and provide a means for more complete on-scene victim care.
In the past decade there have been great advances in medical/rescue care for victims of motor vehicle accidents. Training hours for emergency medical technicians, paramedics, and vehicle rescue technicians have increased dramatically. We have more sophisticated, specialized tools and equipment at our disposal than ever before. Our skills and the procedures we use are more refined. These factors, in addition to interagency cooperation between firefighters and EMS, make us better prepared to handle any type of vehicle rescue.
But we’re not perfect; there’s always more to learn. Consider this basic description of many vehicle rescue scenarios: Rescue and EMS personnel arrive on the scene within minutes of each other. Rescue personnel stabilize the vehicle and control hazards; they create a primary access pathway—they pop the door, displace the roof and windshield—so that medical personnel can begin victim assessment, basic life support, and advanced life support if necessary. The medics put on the rigid collar and apply oxygen therapy. If they’re providing advanced life support they run an EGG, maybe start IVs of 1,000 lactated ringers or normal salines under their high-risk protocol if the victim is in shock or his blood pressure is low. Rescue personnel sever and displace the vehicle roof so that medical personnel can hold cervical traction or slide in a spinal immobilization device. With access to the victim complete, with hazards controlled, and with initial medical attention complete, it’s time to extricate the victim, right?
We conduct a secondary survey of the pelvis area and below and take what we consider to be appropriate actions. If we notice bleeding we control it. If the dash or an operator’s pedal is entrapping the victim, we displace it. If the door is in the way, we remove it. If the seat is jammed forward we slide it back. We hold off on the legs until we start the extrication phase and then we slide the victim out onto the spine board, after which we apply the medical antishock trousers (MAS I ) or splinting devices.
Wait a minute. Take a step back. What about the “hidden fracture”? What about the legs?
The victim may be in severe shock. He may have pelvic injuries. Still want to move him now? Are you certain that sliding the seat back won’t cause further injuries? You’re going to splint the legs after you’ve already moved them several times? The victim may have a blood pressure of 80 systolic. How long will it take for his blood pressure to fall after you bring him from the sitting to the supine position? Not long at all. Still want to move him now?
Remember why you are there —to provide the best possible protection and care to the victim that you can, in every respect! Apply the MAST before you move the victim out of the vehicle. In most cases the victim will arrive at the trauma unit in the same or better condition as he was while sitting up in the vehicle.
Here’s an extrication method that takes into account the “forgotten fracture.” It will shorten your total onscene rescue time and improve the victim’s chances of receiving complete, quality medical care. I’ve used it and found it to be very effective. (Remember that we re in the disentanglement phase of operations. Sizeup, hazard control, and access have already been achieved.)
First, make sure the vehicle is properly stabilized. Today’s vehicles are of unibody construction, so solid cribbing under the A-post and C-post is the most effective method of stabilization.
Second, leave the doors on! If the door on the victim’s side isn’t already opened, unlock it and try manual means. If that’s unsuccessful, use your hydraulic spreader to open it. Use the door as a purchase point for further displacement of the dash and lower Apost.
Next, after you’re certain that your cribbing is properly placed and tight, make a complete cut at the bottom of the A-post as close to the floor as possible. Use your air chisel, sawsall, or hydraulic cutter.
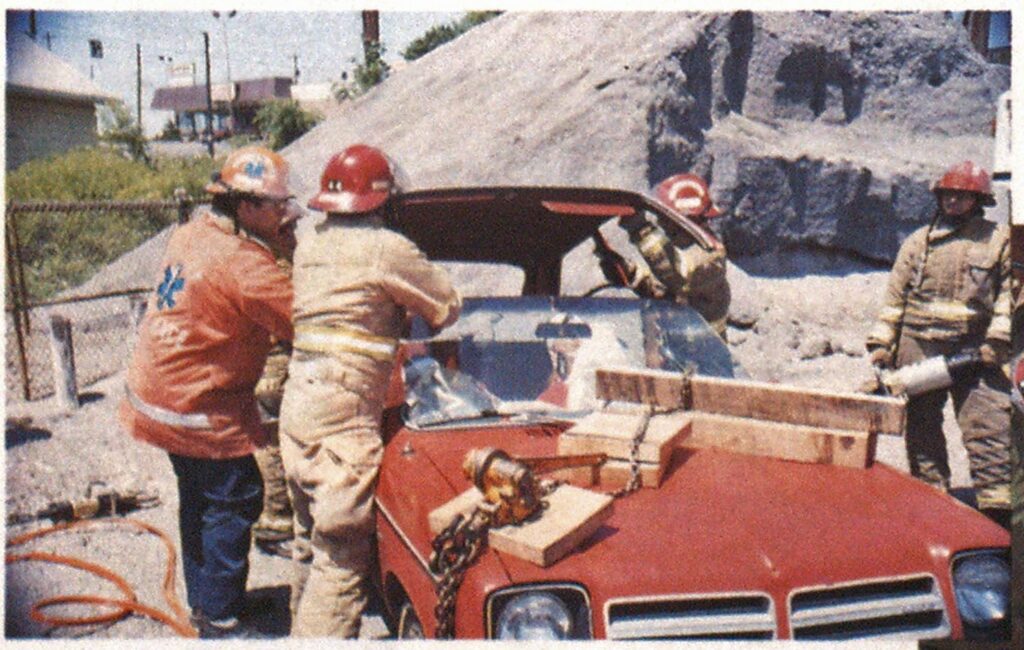
Next, take your single 1 ½-ton, chain come-a-long and secure it to your door chain. Then fill the void space with cribbing. Now position your round, 12-inch rescue log under the front portion of the chain and displace the door and A-post in conjunction with the hydraulic spreader or porta-power. By tightening the come-a-long, the door, A-post, and front end of the vehicle will displace out of your way. Then cut the steering wheel.



(Photos by author.)
Now medical personnel can use the room that you’ve created for leg stabilization before moving the victim. Once the area is clear of sharp material, the MAST can be put on easily and the legs inflated.
If you used this technique, doors wouldn’t be in jeopardy of flying off from the force of hydraulic tools and, most important, hydraulic spreaders wouldn’t be placed in a position that could injure the patient if the sheet metal collapses. Furthermore, hydraulic rams are not used to displace the dash, thereby decreasing the possibility of further entrapment of victims whose legs are in or through the fire wall. And from an operations standpoint, the technique allows for accurate, predictable movement of rescue equipment used to displace the front structural area, especially on frontwheel-drive vehicles.
The virtue of this technique is what it gives us: time, increased safety, and an avenue for better on-site medical care. It developed out of an important philosophy: Don’t do something because it’s always been done that way. Analyze and critique your operations. Be creative. Fay attention to details… and remember the “forgotten fracture.”






