
By Glen Beasley
It is becoming increasingly evident that firefighters are at a much higher risk for cardiovascular disease than workers in any other profession. Researchers continually describe fighting fires as physiologically high risk and suggest that firefighters be treated more as industrial athletes than traditional firefighters. I understand and endorse the best practice of prevention through good health, exercise, effective standard operating procedures, and personal protective equipment; however, the reality of the job, specifically the time and resources needed before fire departments can produce and maintain a healthy workforce, has led me to ask myself, “How can we prepare for the worst if a firefighter collapses and goes into cardiac arrest within the fire building?” This question has been asked by many other firefighters as well because preparing for the worst allows for an effective and a timely response to any situation.
A study conducted in Amsterdam that included 873 people who suffered cardiac arrest found that when bystander cardiopulmonary resuscitation (CPR) was performed, it resulted in a survival rate of 14 percent compared with a survival rate of six percent when no bystander CPR was carried out before the arrival of paramedics.
Taking these figures into account and understanding the CPR survivability scale in which a seven to 10 percent chance of survival is lost every minute without CPR and that an average rescue time of a down firefighter is between 71/2 and 21 minutes, in the best-case scenario, a firefighter has a 25 percent chance of survival if efficient and effective CPR practices are initiated immediately on the firefighter’s removal from the fire building.
CPR Drill: NSWFR vs. Leland FDCPR/FDCAD Method
How do we deliver the very best, time-efficient, medical response to a down firefighter? With this question in mind, I embarked on a validation study supported by Charles Sturt University and my department, New South Wales Fire and Rescue (NSWFR) in Australia. We assessed the effectiveness of a firefighter down cardiac arrest drill (FDCAD), which we had recently discovered and was initially developed by the firefighters of the Leland (NC) Fire Department (LFD). This method appeared to facilitate early CPR for a down firefighter as well as rapid removal of bunker gear and self-contained breathing apparatus (SCBA) while conducting an efficient, well-practiced CPR drill.
This approach was to be compared against the standard NSWFR drill, in which the rescuing firefighters surrounded the firefighter on removal from the fire building and removed all personal protective equipment (PPE) in an unorchestrated manner and then began CPR. The standard procedure is referred to as the NSWFR CPR Drill.
Objectives
The validation study (Beta test) focused on several key outcomes to gain a better understanding of the drill’s efficiencies and downfalls. The goals of Beta testing included establishing a baseline of user performance; establishing and validating user performance measures; and identifying potential design concerns to be addressed to improve efficiency, productivity, trainability, and end-user satisfaction. The Beta test objectives included identifying design inconsistencies and usability problem areas within the firefighter CPR drill such as the following:
- Training errors: failure to educate personnel so they would understand the drill’s functions, requirements, and uses.
- Timing errors: failure to properly carry out the drill within an appropriate timeline consistent with the pathophysiology of cardiac arrest.
- Cardiac arrest identification: the ability of responding firefighters to determine if the casualty is in cardiac arrest and how to respond.
- Efficiency problems: failure to achieve CPR drill efficiency from a physiological standpoint including rate, quality, and depth of compression.
- Fatigue error: failure of the rescuer to maintain efficient CPR because of fatigue created by the drill design.
- Encoding confidence error: failure of personnel to confidently recall and perform the drill posteducation.
- Other equipment: identify potential problems associated with equipment carried by firefighters at a fire scene – such as radios, webbing, truckies’ belts, and so on.
Pretesting Requirements
Prior to the testing day, participants attended a three-hour CPR training course outlining basic CPR, standard firefighter down procedures, and the LFD’s FDCPR/FDCAD procedure being assessed. They also were required to fill out a confidence and encoding survey that assessed their current knowledge of and confidence in performing standard CPR and the NSWFR firefighter down procedure. Four volunteers from the ranks of NSWFR participated in a Beta study session. Testing was conducted at the Charles Sturt University’s Bathurst City campus paramedic training simulation space.

Test Protocol
Measurements pertaining to CPR efficiency were obtained through an accelerometer built into a CPR manikin; it measured the time of the first intervention, heart rate, rhythm, quality, g-force exerted on the patient, and ventilation volume. This information was then downloaded onto a computer for further analysis.
Secondary to this, participants in scenarios were also video recorded and time stamped on completion of set interventions, such as removal from SCBA, to facilitate assessing the speed of disrobing the injured firefighter because of flexibility issues with the manikin and the need for a live participant to take its place.
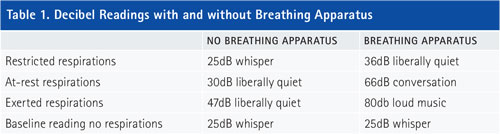
When assessing the ability to confirm cardiac arrest, decibel readings were gathered to identify the sounds of breathing when the casualty withholds breathing, breathing at rest, and breathing when fatigued. This allowed the study to determine if it was reasonable to assess a patient through an SCBA.

Additionally, a watch and a feel test were completed with patients in PPE displaying no, shallow, and deep respirations and rescuing firefighters attempting to distinguish among them.
Measurements were also gathered by biometric shirt and automatic blood pressure cuffs, which record and observe vital signs, fatigue, and the external g-force of rescuers. This allowed us to assess the level of exertion rescuing firefighters sustain throughout the evolutions and the time frame for which they could efficiently maintain rescue efforts while wearing their own PPE.
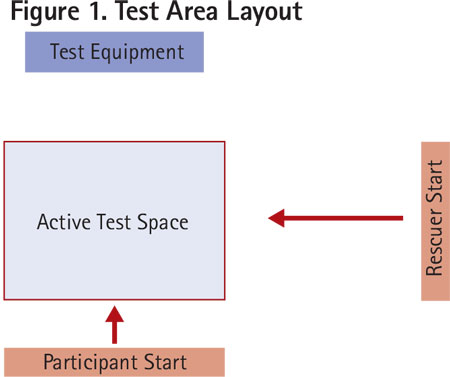
The test space was comprised of an active test box marked in red and two start boxes also marked in red (Figure 1). This allowed a realistic view and time frame for the rescuing firefighter to remove the patient from the fire building and other rescuing firefighters to converge on them to begin the resuscitation.
At the commencement of testing, a baseline test measured the firefighter’s performance in conducting a regular CPR procedure on a manikin. There was then a one-hour rest period between this test and the next one. Three tests were completed: the Baseline CPR method normal CPR; the NSWFR method, the current drill used; and the FDCPR/FDCAD method, the new drill. The FDCPR and FDCAD methods are essentially the same, except that the FDCAD checks for breathing before CPR begins; this is a requirement in Australia.
The Baseline CPR test was conducted on a manikin. Four tests measured the new procedure and standard fire rescue techniques: one test using the NSWFR method on a manikin and the other test on a live person and one test using the FDCPR and FDCAD method on a manikin and the other test on a live person. The manikin tests studied the physiological outcomes for the CPR method tested at the time – e.g., depth of compression. The live person tests studied the time-dependent markers of the CPR – e.g., time to start compressions. There was an hour of rest between tests. At the end of the testing, participants were asked to complete the confidence and encoding questionnaire again so we could assess their perception of the newly learned material.
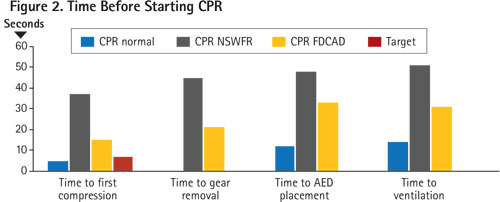
On completion of the testing and collation of the data from the Beta testing, preliminary findings showed significant differences in relation to the three types of CPR drills tested. The time-dependent data showed more than a 50 percent decrease in the time it took to start cardiovascular compressions using the FDCPR/FDCAD method instead of the standard NSWFR drill. There was also a further decrease in all other comparable recorded time-dependent interventions (Figure 2).
Also, it is important to note there is reason to believe that it is possible to reduce time to first compressions by making additional adjustments to task roles within the LFD method because of additional information acquired in posttesting, represented by the set target in Figure 2. This information included idiosyncrasies to the disrobing process – e.g., the hand position when removing the patient’s face mask and communication among rescuers.
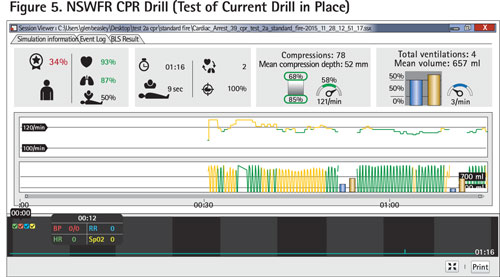
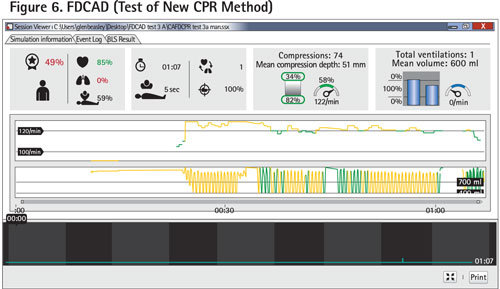
The patient-related clinical data show that minimizing time until the first compression is imperative to increase survivability in any arrest scenario. When compared with a standard CPR drill as a baseline, all three drills outlined similar results pertaining to compression depth, compression rate, and hand placement. Both firefighter down drills matched the International Liaison Committee on Resuscitation (ILCOR) guidelines of a five-cm depth of chest compression and a rate of 100 compressions a minute. The associated scores were assigned by software (QCPR) from data measured through the manikin. Differences in the drills’ efficiency were seen largely because of a CPR score that is mostly a combination of ventilation, intervention time, and compression scores, as seen in Figures 4-6. In the LFD FDCPR/FDCAD test, there was an outlier in which user error of the clinical simulation manikin resulted in no ventilation data being recorded for the FDCPR or the FDCAD method. Unfortunately, this test could not be repeated because of learning biases. Even though this error occurred, there was still a 15-percent increase in the CPR score when comparing the LFD FDCPR/FDCAD and NSWFR methods (Figure 4). This is most likely attributed to the time efficiencies of the drill that allowed compressions to begin before the patient is removed from the firefighting equipment, as seen in Figure 2.
Decibel readings were obtained to determine if a casualty could be assessed through an SCBA. It was assumed that the SCBA mask would act as a funnel, channeling air out of the exhalation valve, causing a rush of air, because of its positive pressure. The decibel readings taken showed the SCBA acted as an amplifier, in turn improving the rescuer’s ability to hear sounds of breathing (Table 1).
Additionally, the watch and feel test reported 98 percent of the rescuing firefighters could identify chest rise and fall and breathing when a hand was placed on the chest and felt little to no impairment from the firefighting ensemble. That air can be felt moving out of the casualty’s SCBA by a rescuing firefighter also when placing an ungloved hand over the exhalation valves on a breathing apparatus mask.
Participants were given surveys to assess their confidence and ability to teach the drills to assess any change pre- and postintroduction to the FDCPR/FDCAD method.
Analysis of Test Findings
Analysis of the confidence and encoding CPR drill data showed an initial preassessment score of equal proportions within neutral and positive bars. This response was expected since the test participants were emergency responders and trained in basic life support annually, even though, when asked to comment, many participants stated, “I did not even know a drill or procedure existed until now,” and, when observed, they seemed unsure of where to begin.
On completion of drill instruction and assessment, the postdrill data outlined a change of 42 percent from being neutral about the drill to viewing it as a positive. Participants’ comments became more positive: “Awesome, much better than what exists now.” These data are shown in Figure 7, which shows the recorded negative, neutral, or positive responses from participants pre- and posttesting.
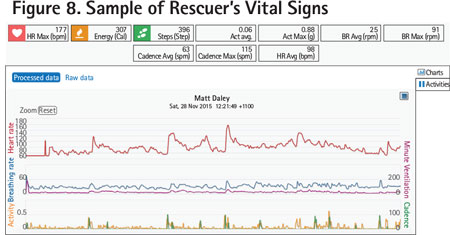
Rescuer physiological and accelerometry measures were acquired during all three drills using the biometric shirt. Although not a key part of the proof of the concept study, the measure of rescuer physiological changes (heart rate, respiratory rate, and minute ventilation) deserves further study. Additionally, there is an opportunity to correlate g-forces as measured by the biometric shirt during CPR with the physiological and time-dependent observed measures. This research has not been conducted anywhere in the world; this study is the first to examine these measures.
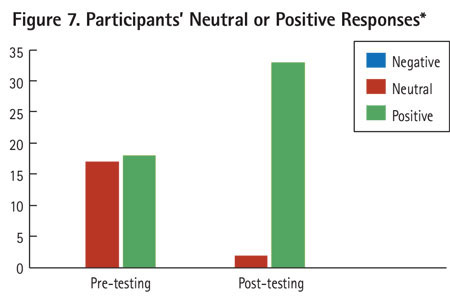 |
| * There was no negative data; therefore, no negative bar is shown. |
The sample output is illustrated in Figure 8. The data show an increase in the rescuers’ vital signs such as heart rate, respiratory rate, and minute ventilation during all CPR drills. There was a further increase when the firefighter was required to wear PPE, although there did not seem to be a decline in CPR efficiency in the short assessment time of the drills. It could be assumed that fatigue would set in at an accelerated rate and rescuers should remove their PPE as soon as reasonably possible to reduce losses in CPR efficiency.
Throughout the study, equipment such as radios, flashlights, webbing, thermal imaging cameras, and utility belts was placed on firefighters throughout the CPR evolutions. This equipment did not cause any restrictions throughout the process. It was important to note that when this equipment is removed, it should be placed away from the casualty, allowing 360° of access to the patient. This 360° of access allows for greater efficiency and the ability to change roles throughout the resuscitation effort.
Our research has shown that the LFD FDCPR/FDCAD method can possibly improve survivability for a down firefighter. It is anticipated that making small alterations to the FDCPR/FDCAD method will positively affect outcomes. Although it is important to note the testing has shown strong trends, additional testing is needed to validate these results. A larger sample size is needed to better represent the firefighting population.
It is also important to understand that this is a multifaceted issue and it is necessary to carry out further improvement and investigations in the areas of firefighting, including firefighter health education, firefighters being physiologically prepared for a response in terms of proactive hydration, fitness, and fatigue management and developing strategies to combat fireground issues such as physiological recovery from the fireground environment and the decontamination of harmful substances – for example, particle contaminants and gases such as carbon monoxide and hydrogen cyanide.
Having an effective, time-efficient method of response, casualty location, patient/load management, and extraction by rapid intervention teams will further increase the rate of survivability if an arrest occurs. If fire departments around the world adopt these measures, they may not only improve chances of survivability when a fellow firefighter has suffered an arrest but, through education, may also lower the occurrence of arrests altogether.
GLEN BEASLEY is a career firefighter with New South Wales Fire and Rescue and a paramedic for the New South Wales Ambulance Service in Australia. He has served for 13 years in the emergency services in volunteer and career capacities within public service and private enterprise. His experience includes urban, suburban, rural, and industrial emergency response. His background includes firefighting, rescue, hazmat, mine rescue, wildland firefighting, emergency medical response, public education, and emergency preparedness. While working as a firefighter, he completed the requirements for a bachelor’s of clinical practice (paramedicine) degree at Charles Sturt University Bathurst.
Firefighter Cardiac Arrest : Chain of Survival
Firefighter Down: Treating Cardiac Arrest
Penn (IN) Firefighters Train for Cardiac Arrest of Fellow Firefighters
Fire Engineering Archives

