
fireEMS ❘ By Kim George
The threat of mass-casualty incidents (MCIs), specifically active shooter events, continues to present an ever-growing challenge for responders. The ability to mitigate them has been a hot topic not only because of their frequency but also because of the tremendous variables that become obstacles in numerous ways. Fire/emergency medical services (EMS) will be on the scene of every active shooter event with injuries, but do these first-out responders carry enough critical EMS equipment (tourniquets, QuikClot®,1 chest seals, and decompression needles, for example) to distribute on scene as quickly as needed? Serious bleeding can take a life in less than 10 minutes.2 Hemorrhage is responsible for 20 percent of trauma-related deaths and is considered preventable.3 To reduce this percentage, expedient equipment and supply deployment are essential, but how available is the equipment currently in the quantities that may be needed?
Dilemma 1: Does fire/EMS arrive on scene to an active shooter event with an adequate amount of life-saving intervention equipment?
The American College of Surgeons has put together a phenomenal Stop the Bleed (STB) campaign.4 This course was derived from the Hartford Consensus committee that developed a list of recommendations to improve survival from an active shooter event.5 The Hartford Consensus committee consisted of surgeons, law enforcement, and various first responder disciplines. It developed and advocates the acronym THREAT: Threat suppression, Hemorrhage control, Rapid Extrication to safety, Assessment of medical providers, Transport to definitive care. A few years later, the American College of Surgeons elaborated on the hemorrhage control aspect of these actions and released the STB campaign.6-8 STB educates laypeople in the skills needed to stop life-threatening hemorrhage. The Hartford Consensus recognized that bystanders at the scene of an active shooter event are the most likely individuals to successfully mitigate life-threatening bleeding.9 (6-8) This point is the catalyst driving initiatives to educate the nonEMS population. The goal eventually is to teach hemorrhage control at a pace similar to cardiopulmonary resuscitation.
The STB course delivers an excellent understanding of managing life-threatening bleeding with direct pressure, wound packing, and the use of commercial tourniquets. (4) Wound packing is undoubtedly something the layperson can improvise with ordinary material (cotton shirt vs. coagulant-impregnated gauze), although hemostatic gauze would have a dramatically enhanced effect.10 Information taught on using tourniquets often presents intriguing responses.
There tends to be a misconception that all interventions can be improvised; the tourniquet, however, is not one of them. When people are dissuaded from using a belt or a shoelace as a field tourniquet, there is typically a fair amount of questioning. As their understanding grows, students buy into the tourniquet concept, but they often voice their concern about the availability of these devices. If they did buy one, would they have it when they really needed it? If not, where would the tourniquets come from? How could or would they be provided when and where they are needed?
Dilemma 2: What information can be shared with STB students that will help them feel more invested with the tourniquet skill?
Tourniquet kits (containing eight tourniquets) are available for purchase through bleedingcontrol.org. Many have been purchased or donated for strategic placement at public sites, generally near mounted automatic external defibrillators (AEDs). This kit offers one option for tourniquet availability, but it may not suffice in a mass-casualty incident
South Lake Tahoe (CA) Fire Rescue (SLTFR) Approach
Nestled in the beautiful Sierra Nevada mountains is an oasis of natural splendor. South Lake Tahoe (SLT) is a gem of Northern California that draws tourists with its phenomenal winter and summertime outdoor recreation. The California/Nevada state line roughly runs the length of the lake. The city sits directly adjacent to the Nevada casino corridor on the south shore, complementing the daytime activities with a nightlife that runs well in the morning hours.
Because of the two peak seasons (summer and winter), the modest 24,000 population of SLT swells to 100,000 to 200,000 plus. This population influx presents a more significant potential for MCI events and a need for community engagement with a bleeding-control program.
SLTFR, my department, taught 11 STB courses during 2018 and continues to schedule more. Student groups have included Boy Scouts, law enforcement, citizen emergency responder teams, Soroptimist International, and the general public. Along the way, STB course students are encouraged to purchase their own tourniquets to have on hand, just in case. But, they do have questions regarding the availability of tourniquets in a major event. The SLT police officers carry tourniquets, but even they ask where more might come from if needed.
The intent behind educating the public is to expedite life-saving interventions knowing that EMS will not be able to get to everyone who is seriously injured as rapidly as is needed to help save their lives. As seen in the October 2018 event in Las Vegas, there were massive life-threatening injuries scattered along a massive radius.11 If an event remotely similar were to occur in Tahoe, the availability of a large number of tourniquets could dramatically impact the number of fatalities. Most ambulances carry tourniquets, but they generally stock only two commercial tourniquets.12 Law enforcement carries one if it opts to do so.13 The bleeding control kits available from bleedingcontrol.org come with eight tourniquets that could also be tremendously helpful, but what if the scene is a distance from these caches? What if more tourniquets are needed? Would personnel be available to collect all available tourniquets from the EMS and law enforcement units and get them to the people in need?

(1) The critical intervention bag is easy to carry. (Photos by author.)

(2) Despite its small size, the bag can carry a significant amount of equipment, including multiple tourniquets.
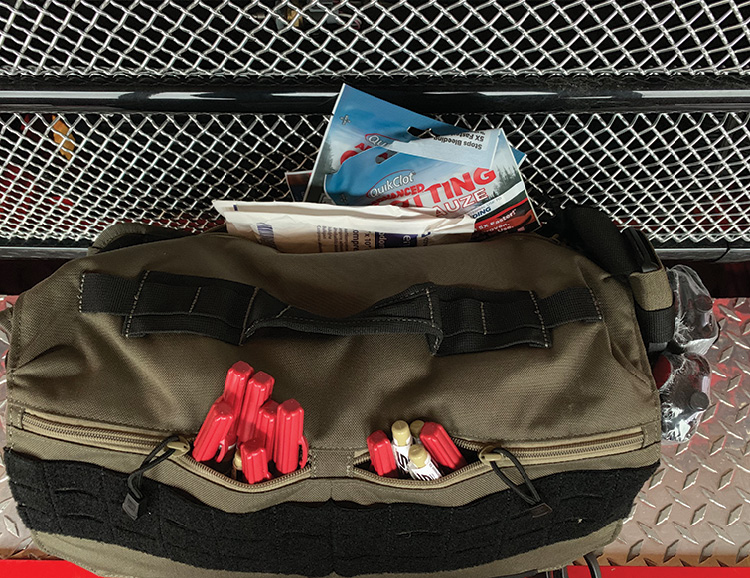
(3) The outside pockets provide space for numerous decompression needles and other items.

(4) The bag easily fits with the tactical vest and helmet cache.
The solution for SLT meant carrying more tourniquets on the engines. Who has space for that, right? Well, as it turns out, a healthy cache of critical gear fits within an 11 × 17 × 4 tactical messenger bag tucked away on our engine with hopes of never being used.
Each bag contains 20 commercial tourniquets, 20 hemostatic dressing packets, 10 chest seals, 14 decompression needles, four trauma shears, a retractable knife, some tape, and a few other small items. We call them “our critical intervention bags” and have them on each apparatus with a plan of not to disturb them unless needed. The earliest expiration date for any of the items in these bags is 2026, which helps with the idea of not disturbing them. When the bag is opened, an inventory sheet that lists the locations of and instructions for the use of all contents becomes readily accessible. A laminated card is attached to the bag and can be easily understood (Table 1).
Since the engines will be at any active shooter event, we are guaranteed that these critical intervention bags will be available on site quickly. They are easily mobile, which makes them available for a force protection team, casualty collection point, or treatment area. Because these events are dramatically different, being able to deploy the bag quickly off a unit that is guaranteed to be on scene provides a level of reassurance about equipment availability.

In an active shooter event, chaos is guaranteed. People will be trying to get away from the hot zone, law enforcement will be attempting to clear those moving out, and fire/EMS will be standing by waiting to make entry. The way this will look varies with each incident; the patient locations are also a dynamic variable. Having multiple bags creates options. One of the most considerable advantages is the concept of distributing equipment as needed without concern about giving away the only or last piece of equipment. As the carrier encounters people who may need equipment, its supply can be handed out on site. This is the point at which the STB course participants become involved. The bag carrier can make a quick round to distribute needed equipment, then walk back through to ensure things are happening as they should or to send another resource into that area for this same task.
Advanced life support providers should ensure that equipment is being applied properly and quickly assess the triage requirement. The on-scene layperson will be a major asset because EMS resources will be immediately overwhelmed. The purpose of the STB courses is to deploy critical intervention bags to distribute tourniquets, providing the laypeople on site with the equipment needed to perform the skills they learned.
During the STB courses, students learn how to use commercial tourniquets. At this point in the training, they are made aware that SLTFR will bring tourniquets to the scene. I explain: “Fire personnel may be reliant on you if you are tending to a patient who is experiencing a life-threatening hemorrhage. You may be the one to save his life. We may hand you the tourniquet, ask you to apply it (if you have made it known that you are familiar with it), and ask you to continue to monitor that patient until we are able to move him toward definitive care.” There is a tendency for the students to reengage and demonstrate immediate interest in ensuring that they have the technique of proper tourniquet application down.
The active shooter event is happening far too frequently in the United States, which is forcing responders to think of these scenarios as a “when,” not as an “if.” Every agency should be working to be as prepared as possible, anticipating the worst. As a smaller quiet mountain town, SLT does not seem to be predisposed for such an event. However, no one is immune. And, with massive population influxes, crowds for a variety of reasons set the stage for a challenging occurrence. For us, these bags provide an opportunity to get a life-saving intervention to those who need it and the hope of community engagement to assist with critical patients who need EMS resources when those resources are taxed to the most extreme level.
The cost of these items is perhaps the most challenging part of this project. For SLTFR, each bag totaled approximately $1,100: The bags are $100; tourniquets, $27 each; QuikClot® packs, $10 each; chest seals, $16 each; decompression needles, $14 each; and other miscellaneous items, a total of $30.
Having fire/EMS apparatus carry an appropriate cache of intervention equipment that can be distributed to where it needs to go and as quickly as it needs to get there minimizes the gap between citizens being able to help and actually helping. There is still a significant amount of work to do: It seems unlikely that we can ever feel we are fully prepared for this worst-case scenario event, but providing this option not only gives the STB-trained laypeople the tourniquets they need to save a life but also addresses the equipment availability concerns at this and other mass-casualty incidents.
References
1. QuikClot® (n.d.). What is QuikClot®? Innovation in hemostasis. Retrieved from: https://quikclot.com/QuikClot/About-QuikClot.
2. Callaway, DW. (2017). Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to Other Austere Environments: Translating Tactical Combat Casualty Care Lessons Learned to the High-Threat Civilian Setting: Tactical Emergency Casualty Care and the Hartford Consensus. Wilderness & Environmental Medicine, 28(Supplement), S140-S145.
, , , , , , , . (2017). Damage Control for Vascular Trauma from the Prehospital to the Operating Room Setting. Front Surg
4. American College of Surgeons (2019). Stop the Bleed. Retrieved from bleedingcontrol.org.
5. Joint Committee to Create a National Policy to Enhance Survivability from International Mass Casualty Shooting Events. (2013). Improving Survival from Active Shooter Events: The Hartford Consensus. Retrieved from: http://bulletin.facs.org/2013/06/improving-survival-from-active-shooter-events/.
6. Jacobs, L and Joint Committee to Create A National Policy to Enhance Survivability from Intentional Mass Casualty Shooting Events. (2016). The Hartford Consensus IV: A Call for Increased National Resilience. Bulletin American College of Surgeons. 101(3) p 17-24.
7. Jacobs, L. (2016). Out of Unspeakable Tragedy Comes Progress in Bleeding Control. Bulletin American College of Surgeons 102(6) 11-16.
8. Jacobs, L and Joint Committee to Create A National Policy to Enhance Survivability from Intentional Mass Casualty Shooting Events. (2015). The Hartford Consensus III: Implementation of Bleeding Control. Bulletin American College of Surgeons 100(7).
9. Bennett, BL. (2017). Tactical Combat Casualty Care: Transitioning Battlefield Lessons Learned to Other Austere Environments: Bleeding Control Using Hemostatic Dressings: Lessons Learned. Wilderness & Environmental Medicine, 28(Supplement), S39-S49.
, , Catastrophic hemorrhage in military major trauma patients: a retrospective database analysis of hemostatic agents used on the battlefield. J R Army Med Corps
11. Clark County Fire Department, Las Vegas Metropolitan Police Department, Federal Emergency Management Agency. (2018). Oct 1 After Action Report. United States. Federal Emergency Management Agency Clark County. retrieved from: https://www.hsdl.org/?view&did=814668.
12. White, E, C Cash, J Augustine, R Fowler. (2016). Tourniquets in Field Management of Active Bleeding. JEMS.
13. Cornelius, B, Campbell, R, & McGauly, P. (n.d.). Tourniquets in Trauma Care: A Review of Application. Journal of Trauma Nursing, 24(3), 203–207.
Kim George, NREMTP, BSN, MBS, has been a firefighter/paramedic for 18 years and is a captain/paramedic for South Lake Tahoe (CA) Fire Rescue, where she has been in a lead role in EMS since 2003. She leads the FTO program and the El Dorado County CQI. George is a registered nurse and has a bachelor’s degree in nursing from Excelsior College and a master’s degree in executive fire leadership with an emphasis in disaster preparedness from Grand Canyon University.

