By Francis Califano
It’s a cool spring evening, and you have just finished the evening meal and settled in for your stint as “house watch.” The bay doors are open, and you lean back in the chair to watch the passersby. Suddenly, a naked man streaks by. You hear a commotion just outside, past your view. The man who just ran past is now engaged in a wrestling match with a parking meter. He is trying with all his strength to dislodge the meter from the ground. The other firefighters join you in trying to corral this person. As you make eye contact with him, you can see rage in his eyes. You try talking to the man while a couple of your colleagues circle around him. He tells you that the meters are trying to control his mind; they told him that they can see through him and that his clothes were radioactive. He lunges at your group; it takes all five of you to control him. The lieutenant calls for the police and emergency medical services (EMS) forthwith.
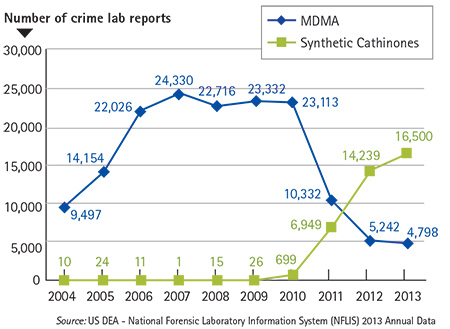
You have just had your first encounter with a person under the influence of a new “designer” drug called “flakka” that has been wreaking havoc in southern Florida. Flakka, a variation of the Spanish word flaca, which means thin, pretty woman, is a synthetic drug similar to ecstasy and bath salts. The active ingredient in flakka is the chemical compound α-PDP (alpha-pyrrolidinopentiophenone), a synthetic stimulant drug of the cathinone class. The U.S. Drug Enforcement Agency (DEA) banned this drug in 2014 and classified it as a Schedule 1 drug; it is considered dangerous and poses a high risk for abuse and dependency. Flakka, sometimes called “gravel,” has been found in parts of Texas, Tennessee, and Ohio, but reports of greatest abuse thus far have come from Florida. Over time, crime lab reports have demonstrated a steady increase in the use of cathinone-based drugs and a corresponding decline in those involving MDMA (molly) (Figure 1).
| Figure 1. Use of MDMA and Synthetic Cathinones in USA |
 |
Symptoms and Characteristics
Flakka, or α-PDP, acts as a norepinephrine-dopamine reuptake inhibitor and can cause a condition of excited delirium in which patients exhibit signs and symptoms ranging from insomnia to hallucinations, paranoia, psychosis, and even death. The drug also causes hyperthermia; body temperatures as high as 106˚F have been reported. The high temperatures lead to nakedness, as users tear off their clothing in a diaphoretic delusional rage. The drug has also been associated with “superhuman strength,” a result of adrenaline surges. Flakka, which usually appears as a white- or pink-colored, rather foul-smelling crystal, can be taken orally, snorted, smoked, or even vaporized (with the use of an e-cigarette cartridge). Vaping is popular with younger users because it gives off no odor, but it increases the risk of overdose because it is very quickly absorbed into the bloodstream.
Complications from abuse of α-PDP result from the user’s extreme state of agitation. During this state, users may harm themselves and others. Other serious medical complications that often have a delayed appearance may result from flakka. Patients who develop a period of agitation can progress into a condition referred to as “excited delirium syndrome” (ExDS), which is to be considered a true medical emergency. Efforts to restrain or control patients with ExDS often add to their complications. As the patient struggles to free himself and flails at your efforts, his increasing hyperthermia can lead to seizures. The combination of elevated body temperature and hyperactive muscle (or muscle activity from seizing) use may lead to metabolic complications. As muscle tissue breaks down, it releases proteins and other by-products into the bloodstream, a process known as rhabdomyolysis. Coupled with dehydration, this process can progress to impaired kidney function, renal failure, and death.
Flakka is typically manufactured overseas in Pakistan, India, and China. It is packaged in one-gram “caches” and sold for roughly $5. These offshore manufacturers make subtle changes in the chemical constituency of the substances in attempts to foil detection by DEA agents. They have been mixed with pricier drugs like cocaine, heroin, and methamphetamine, which can produce unanticipated effects.
Treatment
Once the patient is safe, treatment involves mostly supportive care. Restraints may be needed for safety, to keep patients from harming themselves, you, or your partners. Administer intravenous (IV) fluid if possible. EMS may need to manage agitation and seizures with benzodiazepines (midazolam, lorazepam, or diazepam); haloperidol (or another antipsychotic agent) may be considered, but it may contribute to hyperthermia or cause dysrhythmias. Monitor the temperature, and aggressively treat it with cooling if >102°F. Note: Administration of haloperidol may result in a dystonic reaction, intermittent spasmodic or sustained involuntary contractions of muscles in the face, neck, trunk, pelvis, and extremities. These symptoms are usually transient and can often be successfully managed with the antihistamine medication Benadryl® (diphenhydramine).
Sample treatment guidelines for violent, impaired, and/or excited delirium (ExDS) patients are provided as a sample template for educational and standard of care purposes only. Local, state, and regional protocols may choose different medications based on formulary and practice limitations and local substance abuse patterns (adapted from Greater Broward EMS Medical Directors Association).
Safety
- If the patient is violent or an immediate threat to himself, EMS providers, or bystanders, use physical and/or chemical restraint to protect from harm. Involve law enforcement.
- If restraint is necessary, do not allow prone positioning.
- Exercise additional caution when evaluating any patient subdued by “nonlethal” law enforcement devices (pepper spray, TASER®) prior to arrival.
- If the patient is nonviolent, avoid provoking him. Use verbal tactics to deescalate the situation. Consider removing the patient from a stressful environment.
Assessment: Additional Conditions
- Consider other causes for impairment or violent behavior: psychiatric conditions, drug overdoses, stroke, ethanol alcohol, hypoxia, hypoglycemia, or head injury, for example.
- Typical findings in violent/impaired/ExDS patients include the components of the acronym PRIORITY:
Psychological issues
Recent drug/alcohol use
Incoherent thought processes
Off (clothes) and sweating
Resistant to presence/dialogue
Inanimate objects/shiny/glass – violent
Tough, unstoppable, superhuman strength
Yelling
- ExDS is an extremely agitated, psychotic-like state in which the patient is unable to focus or use any rational thought process. ExDS patients often exhibit elevated temperature, nudity, profuse sweating, and superhuman strength.
- Check blood sugar.
- Measure SpO2.
- Measure body temperature.
- Exercise close observation of any highly agitated or violent patient who suddenly becomes calm.
Treatment
- Medications to manage aggressive/violent behavior (chemical sedation):
- Midazolam (Versed®) in 2-milligram (mg) increments intravenously (IV), intraosseous infusion (IO), intramuscular (IM), intranasal up to a maximum dose of 10 mg. Note: IV administration may pose safety concerns. Consider intranasal or IM administration.
OR
- Lorazepam (Ativan®) 2 mg IV, IO, IM, intranasal; may repeat once (maximum dose is 4 mg).
OR
- Diazepam (Valium®) 5 mg IV, IO, IM, intranasal; may repeat to maximum dose of 20 mg.
OR
- Ketamine 250 mg IM or 2 mg per kg intranasal (requires 100 mg/mL concentration).
OR
- Haloperidol (Haldol®) 5 mg IM or IV; may repeat once (maximum dose 10 mg).
- Consider diphenhydramine (Benadryl®) 50 mg IM or slowly IV.
- Treat blood sugar following hypoglycemia protocol.
- If spot oxygen saturation (SpO2) < 94 percent, administer oxygen to maintain SpO2 greater than or equal to 94 percent.
- If temperature > 100°F, initiate cooling using ice packs to head, axilla, and groin. If temperature > 102°F, cool aggressively using ice packs and wet sheet with airflow across surface. Target temp is less than 100°F; do not overcool as this will result in shivering.
- Once the patient is sedated, establish an IV and administer a fluid bolus of 30 mL per kg of normal saline.
- Initiate cardiac monitoring. Treat arrhythmias according to appropriate cardiac protocols. Note that bradycardia may reflect hypoventilation.
- Measure and monitor capnography.
- In case of cardiac arrest, consider early administration of fluid bolus and bicarb.
- Expedite transport to the closest appropriate facility.
Encounters with patients experiencing drug-induced psychotic episodes pose several challenges. Safety must be your first and foremost concern. Anticipate the unexpected; a calm patient can turn on you rapidly, and a violent patient can quickly become calm (a sign of serious concern). Make the decision to restrain a patient cautiously, and always use restraints appropriately. Determine the differential in your treatment by how the patient is presenting. A naked aggressive patient is not an everyday experience and should be some indication of what you are dealing with. Keep in mind the myriad of other medical conditions that might cause altered mental status.
Endnotes
Glatter, R. “Flakka: the new designer drug you need to know about,” Forbes. April 4, 2015. Online: http://www.forbes.com/sites/robertglatter/2015/04/04/flakka-the-new-drug-you-need-to-know-about/. Accessed June 25, 2015.
National Institute on Drug Abuse. “‘Flakka’ Emerging Trends.” Updated May 2015. Online: http://www.drugabuse.gov/drugs-abuse/emerging-trends. Accessed June 25, 2015.
Greater Broward EMS Medical Directors Association. Current Protocols.www.gbemda.org/protocol. Accessed June 28, 2015.
FRANCIS CALIFANO, BS, EMT-P, CHSP, is an emergency management coordinator for North Shore-LIJ Health System in Manhasset, New York. He is assigned to the Occupational and Environmental Medicine Department, Emergency Management Division. He is a 30-year member of Rescue Hook & Ladder Co. #1 of Roslyn, New York. He is company safety officer and has served as captain of EMS. He has a bachelor of science degree in community services/emergency management from State University of New York, Empire State College. He has been a speaker at FDIC as well as at other national conferences. He is a certified hazardous materials specialist as well as a certified healthcare safety professional.
Personal Harness Use for Firefighter Rescue
RAPID INTERVENTION TEAMS
THE RAPID INTERVENTION TIME LINE AND CREW SURVIVABILITY
Firefighter Survival: Training Minutes : Rapid Intervention Team (RIT) Operations

