By FRANCIS CALIFANO
Scenario: The last event of the summer, “Electric Zoo”-a three-day music festival-is about to kick off on Randall’s Island in New York City near the East River. You attend the morning intelligence and safety briefing; nothing out of the norm is expected. You and your partner have been assigned to one of several utility vehicles and will be working the event with additional support from medic bike patrols and an on-scene first-aid station. In addition, six ambulances will be on site for transport.
The afternoon starts off slowly. Most of the crowd appears to be teenagers, “tweens,” and young adults. You handle a handful of minor aided cases-the usual slips, trips, and falls, with an occasional bee sting. As dusk descends over the concert, you see a change in the crowd; they seem a bit older, and an occasional whiff of cannabis wafts through the air. There is also an increase in the number of revelers who may have been overserved with alcohol. Your radio blares, “Gator 2, respond to the north speaker tower for an unconscious female.” You confirm, “Central Gator 2, one minute, out.”
You arrive on scene to find a female in her 20s on the ground being cradled by a friend. She is semiconscious and extremely diaphoretic. As you begin treating her, someone from the crowd informs you of another patient close by. A young man is being escorted toward you. He appears agitated and not very happy being contained. Backup arrives to assist you and your partner. When you ask the crowd for additional information, one of the bystanders tells you, “It’s probably molly.” Your first thought is, “Who is Molly?” The question should really be “what” is molly?
Molly is street vernacular for “molecule,” a supposedly purer example of the drug 3,4-methylenedioxy-N-methylamphetamine (MDMA) (Figure 1) in powder or crystal form. A resurgence of this drug is based on a misnomer of its being “pure,” leading people to believe it is safer than earlier forms. The Drug Enforcement Administration (DEA) lists MDMA as a Schedule I controlled substance (see sidebar “DEA Schedule I Drugs”).
| Figure 1. Elemental Structure of MDMA |
 |
Chemist Anton Köllisch was the first to synthesize the compound, formerly known as “ecstasy,” in 1912. Its use as a stimulant did not become popular until the 1970s when pharmacologist Alexander Shulgin reintroduced the drug and promoted its benefits to his colleagues. Psychotherapist Leo Zeff touted the drug’s potential to inhibit anxiety and as a means for therapists to facilitate patients revealing their innermost fears. MDMA became a commonly prescribed drug among psychotherapists and soon after migrated out of these psychiatric practices and onto dance floors across Europe. MDMA became fashionable among young adults and jet setters. Often ingested in powder form, molly can cost anywhere from $30 to $50 a hit. Molly users are attracted to the drug’s effects including the following:
- Extreme euphoria.
- Increased energy.
- Feelings of belonging and closeness.
- Heightened sensations (touch, taste, smell, and hearing).
- Increased openness.
- Feelings of love and empathy.
- Bright, intense visual perceptions.
- Musical appreciation.
- Fear dissolution.
- “Profound” thought.
Based on these effects, you can imagine why it has become popular among revelers at modern day “electric music” venues, commonly called “raves.” In recent months, there have been documented fatalities from overdoses of MDMA at such concerts in Boston and New York City.1
PREHOSPITAL CARE
As with any patient, address the ABCs (chest compression, airway maintenance, breathing), ensure an airway, administer appropriate oxygen therapy, and obtain vitals including level of consciousness (air, voice, pain, unresponsive). Additionally, check the blood glucose level, place the patient on a cardiac monitor, and obtain intravenous access. Although billed as pure and perceived as safe, molly can have some substantial adverse effects, which include the following:
- Mild to extreme jaw spasms (trismus).
- Short-term memory loss.
- Confusion.
- Headache; vertigo; and loss of muscle coordination, leading to staggering gait (ataxia).
- Muscle tension.
- Nausea and vomiting.
- Difficulty concentrating.
- “Crash” when coming down.
- Hangover lasting days to weeks.
- Depression and fatigue for up to a week.
- Psychological addiction.
- Panic attacks.
Major complications seen in MDMA overdoses include the following:
- Hyperthermia/heatstroke.
- Dehydration.
- Hyponatremia (low-serum sodium).
- Syndrome of Inappropriate Anti-Diuretic Hormone secretion.
- Hepatitis/liver failure/renal failure.
- Rhabdomyolysis (breakdown of muscle tissue).
- Neurotoxic effects.
- Acute psychosis/severe depression.
- Death.
At the top of the list for MDMA overdoses is hyperthermia, which can result in seizures.2 Seizures, most of which are self-limiting, should be treated with benzodiazepines. Protect the airway, and consider phenobarbital or propofol in patients with refractory seizures. (2) Hyperthermia can be life-threatening and necessitates aggressive cooling measures coupled with fluid resuscitation. Morbidity correlates directly to the degree and duration of hyperthermia. Aggressive cooling should be targeted to reducing patient core temperature to 102˚F. (2) Cooling measures include undressing the patient and applying moistened sheets or blankets to the core of the body and ice packs to the groin and axilla (armpits). As a side note, naloxone (Narcan®) is not effective for reversing overdoses involving ecstasy, Gamma-Hydroxybutyric acid, or cocaine. When an overdose is suspected to involve multiple substances, administration of naloxone can aid in ruling opioids out of the equation.
ROUTES OF ADMINISTRATION AND DOSAGE
MDMA compounds are amines that exist as either free bases or salts. The free bases compounds are volatile. Amphetamine inhalers were originally marketed as nasal decongestants. In theory, MDMA could also be used in this fashion, but the chemistry of MDMA renders it virtually impossible to use by sniffing the vapor.3 Conversely, the MDMA salt compounds are water soluble and therefore can be administered intravenously, orally, or by snorting the powder form. Molly is usually taken orally and is purchased in single-dose capsules or tablets (photo 1), which makes it appear legitimate, hence, “safer.” The capsules/tablets vary in dosage from 50 to 100 milligrams (mg). The common dosage among “rave” users is one to two capsules/tablets.
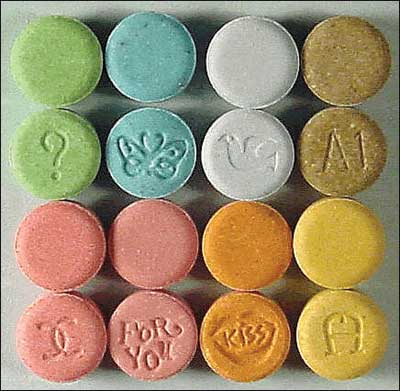 |
| (1) Several types of MDMA tablets. (Photo courtesy of the Department of Justice.) |
PHARMACOLOGY OF MDMA
To better understand the effects of MDMA, review the pharmacology of ring-substituted amphetamines including both the pharmacokinetics and pharmacodynamics of the drug.
MDMA pharmacokinetics. When MDMA is taken orally, the drug is readily absorbed through the intestinal tract and is detectable in blood plasma at peak concentration within two hours of consumption (dose dependent). The drug is metabolized primarily in the liver, where an enzyme designated CYP2D6 is chiefly responsible.4 However, several different enzymes are involved in its degradation,5 and some of them appear to become saturated even at relatively low concentrations of the drug. Consequently, as the dosage is increased and the higher-affinity enzymes are saturated, disproportionately large increases in blood and brain concentrations of the drug occur.6 Therefore, small increases in dosage may carry the risk of significant increases in toxicity.
Elimination of the drug from the body is relatively slow, with a half-life of approximately eight hours, at which point blood levels are difficult to detect. It takes approximately five half-lives for the body to eliminate more than 95 percent of the drug (about 40 hours).
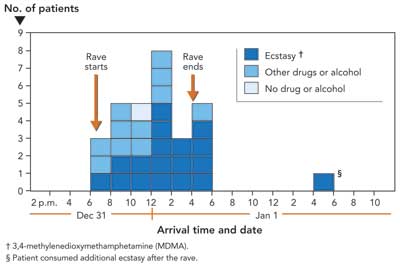
Figure 2 illustrates a Centers for Disease Control and Prevention study of a rave in Los Angeles, California, on December 31, 2009, showing the number, drug use, and arrival times of attendees (total of 30) transported to emergency departments within 12 hours of the end of the event. The highest volume of patients was seen six to eight hours into the event. One patient was transported for trauma; the other 29 were for various drug and/or alcohol intoxications. All but one of the patients arrived at emergency departments within 12 hours of when the rave began.7
| Figure 2. Ecstasy Overdoses at New Year’s Eve Rave-Los Angeles, California, 20107 |
 |
MDMA pharmacodynamics. Research has shown that ring-substituted amphetamines including MDMA act by increasing the release of the monoamine neurotransmitters serotonin and noradrenaline along with small amounts of dopamine from their respective axon terminals. MDMA acts by binding to serotonin, causing it to block the transporters involved in its reuptake. Similar actions-but at a lesser level-take place with the reuptake of dopamine. There is some limited evidence supporting an increased net release of acetylcholine with the use of MDMA, although it is unclear how this might affect humans. The key factors of importance to health care providers are the increased levels of serotonin, which serves as the primary mechanism for the distinctive mental effects of MDMA, and excesses of noradrenaline, which are responsible for the physical effects.
The signs and symptoms of MDMA overdose are self-evident. Knowing what to look for when treating patients of a suspected overdose will aid in your ability to make a differential diagnosis. It may be prudent to do some intelligence gathering before such events to better plan your resource needs.
REFERENCES
1. What is molly? Everything you need to know about the party drug. From http://the week.com/article/index/249040/what-is-molly-everything-you-need-to-know-about-the-party-drug.
2. MDMA Toxicity Treatment & Management. Retrieved from http://emedicine.medscape.com/article/821572-treatment.
3. Shulgin AT. The background and chemistry of MDMA. J Psychoactive Drugs (1986): 18:291 – 308 Medline. Retrieved from http://www.erowid.org/references/refs_view.php?A=ShowDocPartFrame&ID=960&DocPartID=831.
4. Wu D, Otton SV, Inaba T, et al. Interactions of amphetamine analogs with human liver CYP2D6. Biochem Pharmacol 1997;53:1605-12.Medline.
5. Maurer HH, Bickeboeller-Friedrich J, Kraemer T, et al. Toxicokinetics and analytical toxicology of amphetamine-derived designer drugs (“ecstasy”). Toxicol Lett 2000;112-3:133-42.
6. de la Torre R, Farré M, Ortuño J, et al. Non-linear pharmacokinetics of MDMA (“ecstasy”) in humans. Br J Clin Pharmacol 2000;49:104-9.
7. Ecstasy Overdoses at a New Year’s Eve Rave. Los Angeles, California, 2010. Retrieved from http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5922a1.htm.
DEA Schedule I Drugs
Schedule I drugs are defined by the United States Controlled Substance Act (21 CFR 1308.11). The following findings are required for drugs to be placed in this schedule:
- The drug or other substance has a high potential for abuse.
- The drug or other substance has no currently accepted medical use in treatment in the United States.
- There is a lack of accepted safety for use of the drug or other substance under medical supervision.
Except as specifically authorized, it is illegal for any person
- to manufacture, distribute, dispense, or possess with intent to manufacture, distribute, or dispense a controlled substance; or
- to create, distribute, dispense, or possess, with intent to distribute or dispense, a counterfeit substance.
FRANCIS CALIFANO, BS, EMT-P, CHSP, is a 30-year member of Rescue Hook & Ladder Company #1 of Roslyn, New York, where he is a company safety officer and has served as captain of EMS. He is also an emergency management coordinator for North Shore-LIJ Health System, Protective Services in Syosset, New York, assigned to the emergency management division. He has a bachelor of science degree in community services/emergency management from State University of New York-Empire State College. Califano has been a speaker at the Fire Department Instructors Conference as well as other national conferences. He is a certified hazardous materials specialist and a certified health care safety professional.
Fire Engineering Archives

